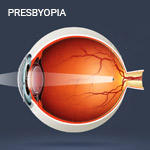
Presbyopia is a loss of accommodative abilities, mostly commonly resulting in reduced near vision in the early stages and is usually, but not always an age-related visual impairment. The gradual decrease in accommodation can have a significant impact on visual clarity and the quality of life. Though not incapacitating if corrected, presbyopia without optical correction results in an inability to perform once effortless near tasks at a customary working distance without experiencing visual symptoms.
Presbyopia has been described as "an irreversible optical failure, an unexplained evolutionary blunder that comes as a psychologic shock." As the amplitude of accommodation diminishes, the range of clear vision may become inadequate for the commonly performed tasks. The impact of this process varies from one person to another and those who are involved in more frequent or more demanding near vision tasks are likely to have greater difficulty. Because the need to read and work at near and intermediate distances is important in all industrialized societies, presbyopia has both clinical and social significance.
Signs and symptoms
The onset of presbyopia is gradual, although blurred near vision signals the onset of presbyopia, the symptoms reach significance only when the patient's accommodative amplitude becomes inadequate for his or her visual needs. Difficulty in performing vocational or avocational activities largely determines when the symptoms of impairment are manifest.
Blurred vision and the inability to see fine detail at the customary near working distance are the hallmarks of presbyopia, yet other symptoms include:
Focusing delays
Ocular discomfort
Headaches
Asthenopia
Squinting
Fatigue or drowsiness
Increased working distance
A need for brighter light for reading
Diplopia
Detection and Prevention
As an age-related condition, presbyopia generally is not considered in the same context as ocular diseases or other disorders that, if left untreated, can have permanent adverse effects on vision or ocular health. Almost everyone eventually will experience some disability due to presbyopia. Among the rare exceptions are a few patients with very small pupils who benefit from increased depth of focus, some who have little need to see fine details at near, and some with antimetropia, who function in a monovision fashion, using one eye for distance vision and the other for near.
Patients typically experience the initial symptoms of presbyopia at an age when more frequent ocular health examinations are recommended because of higher risk for many age-related diseases (e.g., glaucoma, cataract, macular degeneration, diabetes mellitus, hypertension). The responsibility of the optometrist goes beyond identifying and treating the presbyopia that may have precipitated the visit.
Stats and causes
The prevalence of presbyopia is higher in societies in which larger proportions of the population survive into old age. With the aging of any population, unprecedented numbers of patients with presbyopia present to optometrists' offices an attempt to restore clear visual function. Because presbyopia is age related, its prevalence is directly related to the proportion of older persons in the population.
Although it is difficult to estimate the incidence of a chronic condition such as presbyopia, due to its slow onset, it appears that the highest incidence of presbyopia (i.e., first-reported effects) is in persons ages 42 to 44 years of age.
Although age is the major risk factor for development of presbyopia, the condition may occur prematurely as the result of factors such:
Trauma
Systemic diseases
Cardiovascular disease
Drug side effects
Treatment
The evaluation and management of presbyopia is important because significant functional deficits can occur when the condition is left untreated. Furthermore, the onset of presbyopia frequently motivates the individual to seek eye care, presenting the optometrist the opportunity to check for the presence of other disorders, some of which might threaten sight or life. This opportunity underscores the public health benefit of comprehensive optometric care for patients with presbyopia.
As primary eye care providers, optometrists have the expertise to examine, diagnose, treat, and manage a wide variety of eye and vision problems.
For patients requiring other health care services related to systemic conditions detected in the course of their eye examination, the optometrist becomes the point of entry into the broader health care system. Under corrected or uncorrected presbyopia can cause significant visual disability and have a negative impact on the patient's quality of life. Gaining an understanding of the patient's specific vocational and avocational visual requirements helps the optometrist recommend the treatment most appropriate for enhancing visual performance.
A variety of options are available for optical correction of presbyopia, dependent on ocular health, patient's specific vocational and avocational needs, the following spectacle treatment methods for presbyopia include:
Single vision lenses
Anti-fatique lenses
Bifocal lenses
Multifocal lenses
Near progressive lenses
Occupational lenses
All types of corrections for presbyopia represent some visual compromise, compared with normal accommodative ability. Ultimately, the success of treatment depends on the lens power, the optical correction, the specific visual tasks, characteristics of the individual patient, and the appropriate patient education given by the practitioner.
Optical correction with contact lenses (both rigid and soft lens designs) can be used for contact lens correction of presbyopia and include the following:
Monovision contact lenses
Bifocal/ Multifocal contact lenses
Enhanced monovision lenses
Combination of contact and spectacle lens
Many contact lens wearers gain some advantage by combining the use of spectacles with their contact lenses. One common example is the patient who uses contact lenses for distance viewing and adds glasses over the contact lenses for reading. A second example is the patient who has critical near vision tasks for most of the day and chooses to wear contact lenses for near, adding glasses for distance tasks. A third example is the monovision contact lens wearer who sometimes wears glasses to improve binocular vision for the performance of specific tasks. Some contact lens wearers use spectacles to correct residual astigmatism when performing more critical visual tasks.